
It’s tempting to reach for quick-fix protocols when Intestinal Permeability (IP) is suspected or tested for, such as supplementing with extra zinc, glutamine and probiotics, but if the evidence-based risk factors are not addressed and the correct levels of supplementation are not known then protocols are less targeted and therefore less effective.
In his IP protocol, the first of its kind, Dr Leech sets out prescriptive protocols based on the scientific literature. This type of guidance is long overdue and will certainly benefit any practice1.
The terms IP or leaky gut are interchangeable, other terms may include mucosal damage or barrier dysfunction. It is important to recognise that IP is not a condition but a reaction, and a normal homeostatic mechanism. For instance, IP is normal during pregnancy to enable immune system development of the foetus. Therefore, noting a client’s number of full-term pregnancies, for example, is relevant. IP is also an important defence reaction required to wash out pathogenic bacteria entering the digestive tract.
IP occurs when the intracellular proteins holding together the tight junctions of the gut epithelial wall disassemble, caused by the release of zonulin. Zonulin is the only physiological mediator known to regulate IP.
Acute IP is potentially life threatening, and is recognised medically and may accompany, for example, sepsis. Whereas low- grade chronic IP is non-life-threatening and presents frequently in clinical practice.
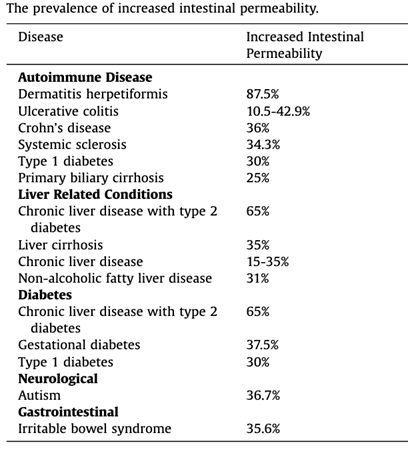
Addressing underlying disease states directly addresses IP and this should therefore be a practitioner’s main objective. IP is both important for overall systemic health and is directly associated with a number of diseases such as autoimmune diseases, and metabolic conditions, such as type 1 diabetes2. Please refer to table 1 below. It is also associated with disease severity and quality of life3.
https://www.sciencedirect.com/science/article/abs/pii/S221295881730160X
Some disease treatments are known to improve IP such as the use of prednisone for Crohn’s disease. Addressing Hashimoto’s disease naturopathically with doses of selenium at 200mcg/day not only results in thyroid antibody improvement within 3 months, but also addresses IP.
Of equal importance is recognising and the subgroups of IP. Refer to figure 2 below.
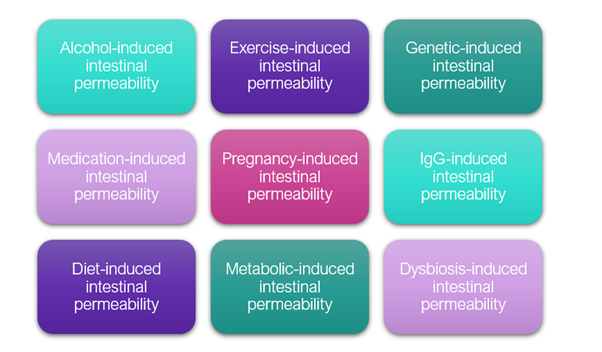
For example, a subgroup of IP is exercise-induced IP. A 2 degree rise in core body temperature has been demonstrated to result in a 3-fold increase in IP due to a lack of blood flow to the intestines, preventing their ability to cool down. When devising strategies for your athletic clients, if 60% of best effort training for 2 hours results in IP, those at risk should modulate their training (ref 4). Additionally, Dr Leech suggests supplementing with curcumin at 500mg twice per day, glutamine at 5g three times per day and colostrum at 900mg twice per day to support training. Although these are higher doses than most practitioners would supplement, his treatment plan is evidenced based and not sufficiently effective at lower doses.
Medication-induced intestinal permeability, for example when NSAIDs (non-steroidal-anti-inflammatory drugs) are taken may be addressed directly by paying attention to other lifestyle factors such as sleep hygiene or suggesting therapeutic yoga to ameliorate symptoms of pain, and supplementing with fish oil and curcumin to address inflammation, and/or by taking PEA (palmitoylethanolamide) supplements at 300mg per day, or Lactoferrins at 250mg twice per day five days prior to the use of NSAIDs as prevention.
Risk factors for IP
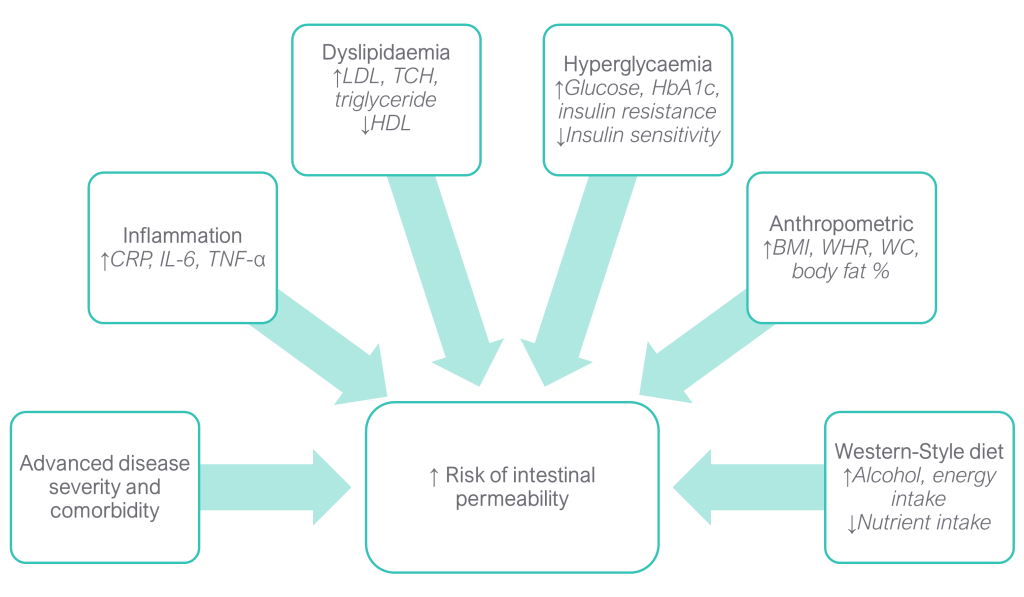
Dr Leech’s research has identified a number of risk factors for IP. Some of the strongest risk factors include elevated levels of proinflammatory markers, dyslipidemia, hyperglycemia, insulin resistance, and anthropometric measurements resembling obesity. These factors can lead to damage in the intestinal lining and promote inflammation, resulting in increased permeability. Additionally, advanced disease severity, comorbidity, and the consumption of a Western-style diet have been identified as significant contributors to altered intestinal integrity. When combined with multiple disease states or other environmental risk factors, the risk of IP becomes even higher. It is noteworthy that several of the identified risk factors, such as anthropometric measurements and biomarkers, are not directly related to intestinal health but rather indicate a metabolic-like condition that may also impact gut integrity.
Other variables to consider, include:
- Modifying the diet, as a Western-style diet high in fat, sugar and fructose and low in fibre diet predisposes towards IP. Focus would therefore be on reducing alcohol, gluten and dairy (ref 1). Challenge clients to eat 30 different fruits and vegetables, nuts, seeds and grains each week.
- Avoiding acoustic stress where possible as a loud noise environment may contribute towards IP.
- Rebalancing the gut microbiota, stool tests are invaluable to analyse the gut microbial profile and gut health can be supported through dietary changes and targeted supplementation.
- Addressing psychological stress and suggesting protocols to ameliorate stress including breathwork, managing workload, appropriate exercise, yoga and meditation and suggesting appropriate supplements, such as L theanine or adaptogenic herbs such as ashwagandha or rhodiola rosea.
Further, the level of advanced degree severity appears to be exacerbated by the presence of dysbiosis, inflammation and glucose metabolism disorders which can be directly addressed. Approximately 1 in 3 individuals experience intestinal permeability in conditions such as autoimmune diseases, please see table 1 above.
When testing for IP, it is important to understand that there is no gold standard, but the two most useful tests to use are measuring the levels of zonulin in stools and measuring the ratio of lactulose to mannitol in urine. Please note that zonulin is released by many cells in the body, including liver and heart cells, so stool zonulin levels rather than blood levels are a more targeted and accurate assessment of IP. In the lactulose/mannitol test, mannitol is readily absorbed whereas lactulose is poorly absorbed, so where IP is present lactulose levels will rise, reflected in the recorded ratio between the two sugars. Both tests may be used together. Stool zonulin is elevated in early disease development as it is an acute phase reactive protein and may be a useful aid to detect early disease state, and the lactulose/mannitol test may be used if a disease state is already identified.
Other tests include the lipopolysaccharide (LPS) test. Lipopolysaccharides are derived from the cell walls of gram-negative bacteria and can be measured in the blood and stool. Look for specific bacteria such as hexa-LPS producing bacteria, such as citrobacter freundii and klebsiellae, amongst others, which are more pro-inflammatory than other LPS compounds.
Food sensitivity testing is a useful measure of IP as a high number of foods with an elevated IgG antibody immune score on a report indicates a high degree of gut permeability. A beneficial protocol involving the selective removal of elevated foods, whilst also addressing nutritional and supplement repair protocols to the gut wall, can improve both tolerance to foods and directly address inflammation and IP. Testing prevents clients being on unnecessarily restrictive diets, which is of vital importance to gut microbiota balance and diversity.
Improving the health and function of the protective mucus barrier, will directly address IP. This can be achieved through testing and removing those foods that are stimulating an immune response while focusing on functional foods and supplements that support the enrichment of the mucus barrier. Strategies may include the use of multi strain prebiotics, FOS (Fructo-Oligosaccharides), GOS (Gluco-Oligosaccharides), resistant starches including cooked and cooled potatoes and rice, and supplementing with vitamin A, vitamin D, zinc and glutamine.
A varied, high fibre diet is essential. If there is insufficient fibre from plant sources, then specific microbes such as akkermansia municiphilia will feed on mucin as a food source and degrade the mucin layer. Actively selecting functional foods, such as chestnuts, pomegranates and blackberries high in ellagic acid, will support anti-inflammatory probiotic species such as 3-indolepropionic acid producing bacteria (IPA).
Testing for IP provides accurate diagnoses so protocols may be evidence-based. Of a survey of 589 adults, 90% of participants wanted to be tested and 93% stated that if tested they would be more likely to adhere to suggested protocols. Engaging in open communication with clients will determine their desires and expectations and result in a frank discussion regarding financial costs in the short term for long term health benefit.
In his protocol (please scan above), Dr Leech focuses on 8 recognised domains of treatment for clients with IP, whilst detailing the evidence behind their use, their efficacy, and potential benefits and harm. Please refer to figure 4 below.
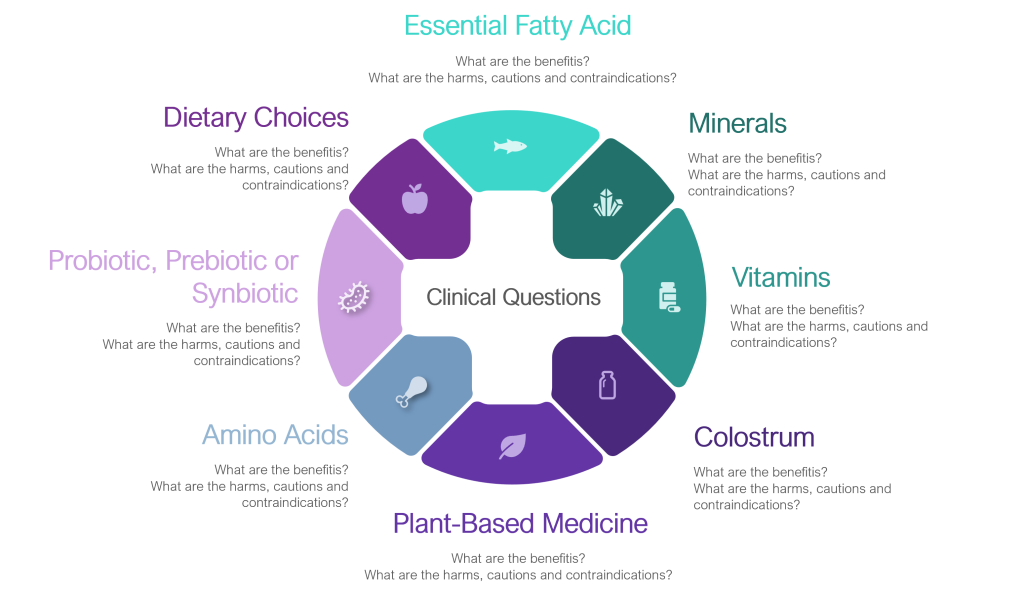
These include the use of essential fatty acids, of minerals, vitamins, colostrum, plant-based amino acids, the grouping of prebiotics, probiotics and symbiotics, and dietary choices.
Based on his protocol, Dr Brad Leech provides practical evidence-based recommendations, such as reducing alcohol to no more than 10 standard alcoholic units per week and no more than 4 units per day, as opposed to a typical recommendation of simply ‘reducing alcohol consumption’.
If a client is clinically obese then restricting the diet by intermittent fasting, may in the short-term be a practical strategy to support IP management. Helping a client reduce their BMI from 43 to 36 has been evidenced to improve IP.
Clients with IP may be able to tolerate gluten, but only small, prescribed amounts and all clients should be low gluten as a rule due to its disruptive effect on zonulin.
Saccharomyces Boulardii has the most profound effect of the probiotic supplements but only if taken for a minimum of 3 months. With regards to other probiotics, good food sources containing multiple species may be recommended such as kefir, kombucha, live yogurts and other fermented foods.
With regards to key amino acids, the research suggests the use of lactoferrin and glutamine at relevant dose levels and the mineral zinc.
In conclusion, a detailed client history will establish underlying health conditions that predispose towards IP and can be directly addressed. Measuring IP with relevant testing supports patient compliance, and identifying and addressing risk factors contributing towards IP will direct targeted treatment recommendations. These recommendations are clearly set out in the IP treatment protocol.
Please register to access Dr Brad Leech’s webinar on the Advancements in the Diagnosis and Treatment of Intestinal Permeability, alongside his webinar slides and references.
References
- Leech, B., Schloss, J., & Steel, A. (2019b). Treatment Interventions for the Management of Intestinal Permeability: A Cross-Sectional Survey of Complementary and Integrative Medicine Practitioners. J Altern Complement Med, 25(6), 623-636. doi:10.1089/acm.2018.0374
- Visser, J., Rozing, J., Sapone, A., Lammers, K., & Fasano, A. (2009). Tight junctions, intestinal permeability, and autoimmunity: celiac disease and type 1 diabetes paradigms. Ann N Y Acad Sci, 1165, 195-205. doi:10.1111/j.1749-6632.2009.04037.x
- Leech, B., McIntyre, E., Steel, A., & Sibbritt, D. (2021). The Subjective Well-being and Health-Related Quality of Life of Australian Adults with Increased Intestinal Permeability and Associations with Treatment Interventions. The Journal of Alternative and Complementary Medicine. doi:10.1089/acm.2021.0202
- Costa, R. J. S., Snipe, R. M. J., Kitic, C. M., & Gibson, P. R. (2017). Systematic review: exercise-induced gastrointestinal syndrome-implications for health and intestinal disease. Aliment Pharmacol Ther, 46(3), 246-265. doi:10.1111/apt.14157
Diagnostics tests from CNSLab
Ready to get a food sensitivity test?
Browse our FoodPrint® home to lab test kits to find the most suitable option.


